Advertisement
Advertisement
January/February 2025
Revascularization of Complex Coronary Artery Disease in Elderly Patients
A patient-centered approach to managing, discussing, and treating complex coronary disease is paramount to ensuring optimal individualized outcomes for older patients.
By Eric Rothstein, MD, and Hannah Chaudry, MD
A principal challenge of practicing geriatric medicine is the opportunity to care for older adults with diverse functional capacities.1 As chronic comorbidities increase in prevalence with an aging population, all physicians, including interventional cardiologists (ICs), need to understand the nuances of caring for a patient population with a wide range of frailty and goals for care.1,2 Age bias interferes with evidence-based health care at all levels of medical training. Multiple studies demonstrate that medical students presented with clinical vignettes surrounding surgical management of breast cancer are less likely to offer a patient-centered approach to older adults.3,4 This problem does not improve with experience and training, as studies evaluating decision-making among surgeons reveal that they are less likely to offer appropriate evidence-based strategies to elderly patients or even engage in shared decision-making,5,6 with many recommendations made based predominantly on the “eyeball test.”7 The effects of ageism and age-related bias also permeate into cardiology, as older hospitalized patients are less likely to even be offered appropriate noninvasive and invasive ischemic evaluation than younger patients.8,9
ICs are routinely faced with the decision of whether to offer complex percutaneous coronary intervention (PCI) as an option for management of coronary artery disease (CAD) in older patients. Performing the procedure itself oftentimes is simpler than having a patient-centered discussion focused on whether to operate in the first place. It is easy for even experienced clinicians to become lost in conflicting evidence, models, and risk calculators when discussing the nuances of potential risks and benefits of PCI and putting these into context with other management strategies, such as coronary artery bypass grafting (CABG) versus medical therapy. Further compounding the difficulty of these discussions in older adults is attempting to incorporate this risk/benefit calculation into a decision that aligns with the patient’s overall goals of care.
In general, when evaluating goals for care, elderly patients prioritize staying independent, avoiding nursing homes, preserving quality of life (QOL), and symptom improvement considerably more than living longer.10 Unfortunately, in all major trials evaluating revascularization for CAD, these are never treated as primary endpoints. Even SENIOR-RITA, a strategy trial that focused exclusively on patients aged > 75 years presenting with non–ST-segment myocardial infarction (NSTEMI), used a traditional primary composite endpoint of cardiovascular death and MI rather than any of the previously mentioned outcomes shown to matter more to older patients.11 Interestingly, this trial showed that an invasive strategy was associated with a reduction in repeat hospitalizations for recurrent nonfatal MIs and repeat trips to the cardiac catheterization laboratory for coronary angiography or PCI at a later date,11 outcomes that again are arguably more important for elderly patients than living longer.
As physicians tasked with managing patients with complex CAD, our job is so much more complex than simply learning how to perform a DK crush or a reverse CART (controlled antegrade and retrograde tracking). It is our responsibility to honor and uphold each individual patient’s values and preferences and engage them in shared decision-making to achieve a consensus surrounding treatment strategies that are in line with both a patient’s risk tolerance and their goals for care. As fitness and frailty levels in older adults correlate very poorly with individualized patient goals for care,10 it is paramount for the IC as part of a high-functioning heart team to not only elucidate an older patient’s individualized goals for care but also advocate for them.12 This all must be taken into account when considering indications for potential outcomes and safely executing PCI in elderly patients, regardless of complexity.10,13,14
DISCUSSING RISKS AND BENEFITS
Older adults have the highest burden of CAD and the disease spectrum is often the most complex; however, they are less likely to be offered appropriate revascularization. Many of the treatment gaps among older patients may be explained by underrepresentation in clinical trials.15 Regardless, the 2021 American College of Cardiology/American Heart Association/Society for Cardiovascular Angiography & Interventions guidelines place a class I indication on making decisions surrounding revascularization, which should be patient-centered and considerate of patient preferences and goals.16
The conversation surrounding the potential benefits of PCI with elderly patients should be relatively familiar for clinicians, as the overwhelming majority of studies published examining the benefits of revascularization in elderly patients compared to younger patients have found that elderly patients derive just as much benefit from revascularization as their younger counterparts. Specifically, in an analysis of elderly patients in the GRACE registry, the Italian Elderly ACS study, the After Eighty study, and the TACTICS-TIMI 18 study, invasive management of ACS demonstrated not only a reduction in subsequent MI and hospitalization but also a significant mortality benefit.12,17-19 Although these trials included CAD of all complexity levels, because extent of benefit from PCI is predominantly linked to the magnitude of relief of ischemic burden20,21 rather than the specific characteristics of the lesion and associated procedural difficulty, these results are still applicable to patients presenting with complex CAD. In the elderly, stable ischemic heart disease population with highly complex disease (chronic total occlusions [CTOs]), it has been demonstrated that patients aged > 75 years derived just as much benefit from revascularization regarding improvements in angina frequency, physical limitations, and QOL, all of which are associated with outcomes that appear to matter to most elderly patients.22
Although benefits are clear, discussions about risks associated with PCI in complex CAD with older patients, should be altered substantially from the discussions a clinician would have with a younger patient. Complications during PCI are far more prevalent and severe in older patients than younger patients. To our knowledge, in every study, registry, or sample of patients with CAD, regardless of the presentation or treatment strategy, increasing age is associated with worse outcomes. All contemporary scoring systems used for prognosticating outcomes in patients presenting with acute coronary syndromes (TIMI [thrombolysis in MI] and GRACE [Global Registry of Acute Coronary Events] scores), undergoing CABG (Society of Thoracic Surgeons score and EuroSCORE II), or undergoing complex PCI (UK-BCIS CHIP, PROGRESS-CTO Complications, OPEN-CLEAN, and SYNTAX II) show that advanced age is associated with worse outcomes. Although there are numerous reasons for a physician to defer offering “high-risk” invasive procedures to elderly patients, physicians are overwhelmingly concerned both with the increased risk of complications and the diminished ability of a patient to recover from a complication.7,23 Although frailty does not typically affect an individual patient’s goals, it does indeed impact the risk of post-PCI complications independent of age.24 Unfortunately, the diversity of patient frailty and comorbidities in the elderly can make risk-stratifying tools less reliable in older patients.25 Studies evaluating outcomes and validating scoring systems in complex and high-risk interventional procedures have such heterogeneous and varied inclusion criteria that, while they might work on a population basis, it becomes challenging to apply them to an individual patient.26-28 Even scoring systems stratified to attempt evaluation of the risk of a single complication (perforation) in a single subtype of extremely complex lesions (CTOs) are limited by the significant variability in both patient characteristics, algorithms, and techniques utilized, as well as operator ability.28-31
When evaluating complex versus noncomplex PCI in elderly patients, it is unsurprising that increased-complexity PCI was associated with a higher risk of complications, with an absolute increased risk of major adverse cardiac events (MACE) of 6.4%.32 For reference, the SYNTAX trial that evaluated the effect of lesion complexity on outcomes in all-comers (albeit in a different era of PCI and with different definitions of lesion complexity) showed an absolute difference of 9.8% in MACE between high and low SYNTAX score groups in patients who underwent PCI.33 Additionally, the SYNTAX trial also indirectly demonstrated the effects of both institutional and individual operator skill set variability on outcomes (Figure 1). All these factors further complicate efforts to apply data from large trials consisting of different operators to the patient in front of a clinician.34 In the end, while these tools work well on the population level, it is challenging to use them to provide anything more than a very rough estimate of risk when discussing potential outcomes with an individual elderly patient.

Figure 1. Outcomes of the SYNTAX trial stratified by site, with size of circle adjusted to the number of patients enrolled at each site, demonstrating the marked variability in both PCI and CABG outcomes at various enrolling sites. MACCE, major adverse cardiac and cerebrovascular events. Courtesy of Dr. Bill Lombardi.
When trying to present a balanced case for choosing between PCI and CABG, it is important to remember that in the most recent major trial comparing PCI to CABG (FAME 3), the primary endpoint was once again composed of the traditional MACE composite of death, stroke, MI, and repeat revascularization, for which CABG demonstrated superiority.35 Interestingly, when evaluating prespecified QOL outcomes in this study that correlate better with those valued by older patients, physiology-guided PCI demonstrated earlier improvement in QOL with similar symptom relief at 1 year to CABG.36 To our knowledge, no major study has defined “prohibitive risk” for PCI, and all of this available evidence, while challenging to digest, is essential for individualized patient care and highlights the importance of shared decision-making. Ultimately, despite these challenges, we advocate for utilizing a multidisciplinary heart team approach to incorporate a broad base of perspectives to arrive at an ideal decision for the patient.
TECHNICAL CONSIDERATIONS
There are no technical changes to a complex PCI that are required simply because one is operating on an elderly patient. Although the prevalence of coronary calcium and vessel tortuosity are increased in elderly patients, there is no need to alter strategies for plaque modification based solely on patient age.37
However, one must be mindful of the increased bleeding risk in elderly patients. In all contemporary models and scoring systems evaluating the risk of bleeding during PCI (DAPT, PRECISE-DAPT, PARIS Score, and ARC-HBR),38-41 advanced age is one of the strongest predictors of major bleeding events. For this reason, clopidogrel is typically the preferred P2Y12 inhibitor for complex PCI in elderly patients. Additionally, proficiency in using the radial approach, as well as troubleshooting commonly faced challenges in radial PCI, allows operators to reduce the risk of bleeding from femoral access complications. Oftentimes, the femoral approach is necessary and even safer for complex cases, so we recommend meticulous attention to detail with the use of both fluoroscopic and ultrasound guidance, despite the conflicting evidence published surrounding any improvements in safety.42,43
Additionally, from a pharmacology perspective, operators must consider the slower metabolism of drugs routinely administered for conscious sedation and the increased risk of a “paradoxical reaction” with the associated dangers of inadvertent gear removal at critical points during the procedure, and they must be mindful of the underlying theme of “start low and go slow.” During complex PCI in elderly patients, time on table is a limited resource, and operators should remember that improving efficiency through adequate preparation and planning, rapidly cycling through different strategies, and even pursuing investment procedures such as STAR (subintimal tracking and reentry) (Figure 2) when appropriate can help improve the safety of a case.

Figure 2. Octogenarian presenting with anterior STEMI due to acute left anterior descending artery occlusion (A). Flow restored after angioplasty (B) with resolution of angina and ST elevations; however, after stent deployment, a large diagonal branch was lost, again resulting in recurrence of ST elevation and severe angina with accompanying agitation that was challenging to manage with sedation. Rewiring of the branch was challenging; however, the subintimal space of the diagonal was wired with a medium-weight, jacketed wire through an angled microcatheter that was subsequently knuckled forward for STAR into the true lumen (C), followed by angioplasty (D), and final kissing balloons to restore flow to the artery (E), with complete resolution of ischemic symptoms.
Finally, operators must understand that CABG as a bailout may not be an option as the risk is simply too high. For this reason, PCI operators are required to be perseverant and creative in their methods for tackling complex cases that are typically referred for surgery in younger patients. Specifically, this has been seen in operators utilizing equipment either “off label” or adapting techniques that were developed for alternative purposes to approach complex lesions in elderly patients (Figure 3).
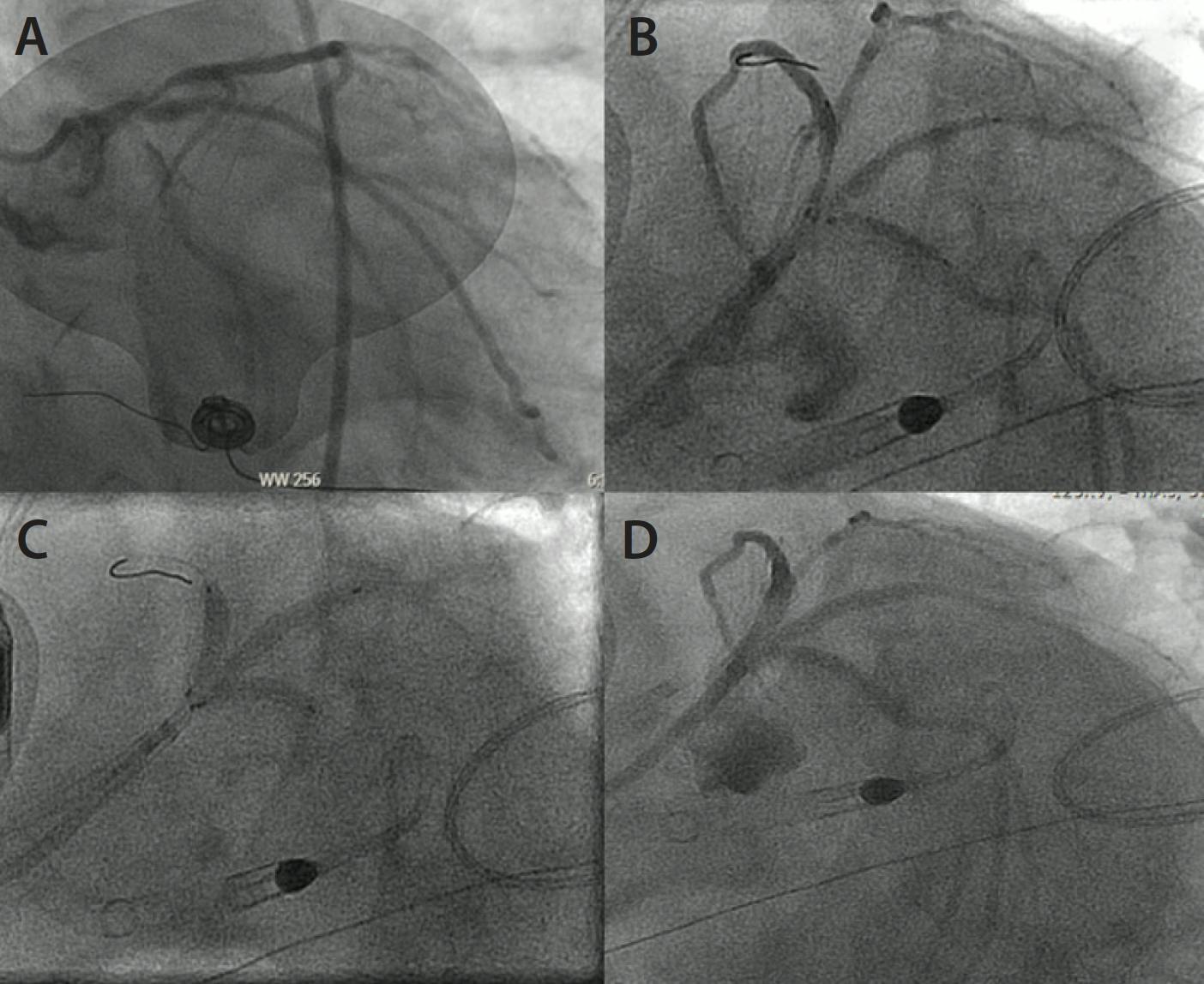
Figure 3. Adaptation of “ping-pong” guide technique typically used for perforation management to treat a nonagenarian with severe aortic stenosis presenting with cardiogenic shock due to lateral STEMI with high-grade distal left main trifurcation disease (A). The patient was rapidly treated with simultaneous “triple kissing” stents (B, C) delivered through dual guide catheters to restore flow to all territories (D) and stabilize the patient.
CONCLUSION
Most medical students learn the principle of nonmaleficence in their first few weeks of education, with some even repeating the renowned Latin phrase “primum non nocere” (first, do no harm) in their white coat ceremonies. This overarching paradigm has been called into question in the field of bioethics, with experts arguing that beneficence (first, do good) takes precedence morally over nonmaleficence in medicine.44 In contemporary medical practice, the shift from paternalism to a respect for patient autonomy has led to individualized and more ethical medical care.45,46 In keeping with the spirit of prioritizing patient autonomy, when discussing revascularization strategies in complex CAD outside of situations of medical futility, it is not our place as physicians to decide for our patients whether they should undergo the risk of complex revascularization, regardless of their age or frailty. However, it is our duty to use our expertise to adequately inform our patients of expected risks and benefits to the best of our ability and help our patients select a treatment strategy that best aligns with their personal goals for care using shared decision-making as part of a high-functioning heart team.
1. Rentsch S, Vitale CA, Zietlow K. Prioritizing geriatrics in medical education improves care for all. Med Educ Online. 2022;27:2105549. doi: 10.1080/10872981.2022.2105549
2. Cesari M, Marzetti E, Thiem U, et al. The geriatric management of frailty as paradigm of “the end of the disease era”. Eur J Intern Med. 2016;31:11-14. doi: 10.1016/j.ejim.2016.03.005
3. Madan AK, Cooper L, Gratzer A, Beech DJ. Ageism in breast cancer surgical options by medical students. Tenn Med. 2006;99:37-8, 41.
4. Madan AK, Aliabadi-Wahle S, Beech DJ. Ageism in medical students’ treatment recommendations: the example of breast-conserving procedures. Acad Med. 2001;76:282-284. doi: 10.1097/00001888-200103000-00019
5. Dharmasukrit C, Ramaiyer M, Dillon EC, et al. Public opinions about surgery in older adults: a thematic analysis. Ann Surg. 2023;277:e513-e519. doi: 10.1097/SLA.0000000000005286
6. Peake MD, Thompson S, Lowe D, Pearson MG. Ageism in the management of lung cancer. Age Ageing. 2003;32:171-177. doi: 10.1093/ageing/32.2.171
7. De Roo AC, Vitous CA, Rivard SJ, et al. High-risk surgery among older adults: not-quite shared decision-making. Surgery. 2021;170:756-763. doi: 10.1016/j.surg.2021.02.005
8. Bond M, Bowling A, McKee D, et al. Does ageism affect the management of ischaemic heart disease? J Health Serv Res Policy. 2003;8:40-47. doi: 10.1177/13558196030080010
9. Dudley NJ, Bowling A, Bond M, et al. Age‐ and sex‐related bias in the management of heart disease in a district general hospital. Age and Ageing. 2002;31:37-42. doi: 10.1093/ageing/31.1.37
10. van der Klei V, Drewes YM, van Raaij BFM, et al. Older people’s goals of care in relation to frailty status-the COOP-study. Age Ageing. 2024;53. doi: 10.1093/ageing/afae097
11. Kunadian V, Mossop H, Shields C, et al. Invasive treatment strategy for older patients with myocardial infarction. N Engl J Med. 2024;391:1673-1684. doi: 10.1056/NEJMoa2407791
12. Nanna MG, Sutton NR, Kochar A, et al. A geriatric approach to percutaneous coronary interventions in older adults, part II. JACC Advances. 2023;2:100421. doi: 10.1016/j.jacadv.2023.100421
13. Coylewright M, Shepel K, Leblanc A, et al. Shared decision making in patients with stable coronary artery disease: PCI choice. PLoS One. 2012;7:e49827. doi: 10.1371/journal.pone.0049827
14. Perpetua EM, Palmer R, Le VT, et al. JACC: Advances expert panel perspective: shared decision-making in multidisciplinary team-based cardiovascular care. JACC Adv. 2024;3:100981. doi: 10.1016/j.jacadv.2024.100981
15. Kumar S, McDaniel M, Samady H, Forouzandeh F. Contemporary revascularization dilemmas in older adults. J Am Heart Assoc. 2020;9:e014477. doi: 10.1161/JAHA.119.014477
16. Lawton JS, Tamis-Holland JE, Bangalore S, et al. 2021 ACC/AHA/SCAI guideline for coronary artery revascularization: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2022;145:e18-e114. doi: 10.1161/CIR.0000000000001038
17. Tegn N, Eek C, Abdelnoor M, Aaberge L, et al. Patients aged 80 years or older with non-ST-elevation myocardial infarction or unstable angina pectoris randomised to an invasive versus conservative strategy: angiographic and procedural results from the After Eighty study. Open Heart. 2020;7:e001256. doi: 10.1136/openhrt-2020-001256
18. Savonitto S, De Servi S, Petronio AS, et al. Early aggressive vs. initially conservative treatment in elderly patients with non-ST-elevation acute coronary syndrome: the Italian Elderly ACS study. J Cardiovasc Med (Hagerstown). 2008;9:217-226. doi: 10.2459/JCM.0b013e3282f7c8df
19. Avezum A, Makdisse M, Spencer F, et al. Impact of age on management and outcome of acute coronary syndrome: observations from the Global Registry of Acute Coronary Events (GRACE). Am Heart J. 2005;149:67-73. doi: 10.1016/j.ahj.2004.06.003
20. Patel KK, Spertus JA, Chan PS, et al. Extent of myocardial ischemia on positron emission tomography and survival benefit with early revascularization. J Am Coll Cardiol. 2019;74:1645-1654. doi: 10.1016/j.jacc.2019.07.055
21. Morici N, Alicandro G, Ferri LA, et al. Residual SYNTAX score and one-year outcome in elderly patients with acute coronary syndrome. CJC Open. 2020;2:236-243. doi: 10.1016/j.cjco.2020.03.005
22. Nguyen DD, Gosch KL, El-Zein R, et al. Health status outcomes in older adults undergoing chronic total occlusion percutaneous coronary intervention. J Am Heart Assoc. 2023;12:e027915. doi: 10.1161/JAHA.122.027915
23. Waldo SW, McCabe JM, O’Brien C, et al. Association between public reporting of outcomes with procedural management and mortality for patients with acute myocardial infarction. J Am Coll Cardiol. 2015;65:1119-1126. doi: 10.1016/j.jacc.2015.01.008
24. Murali-Krishnan R, Iqbal J, Rowe R, et al. Impact of frailty on outcomes after percutaneous coronary intervention: a prospective cohort study. Open Heart. 2015;2:e000294. doi: 10.1136/openhrt-2015-000294
25. Kuplay H, Bayer Erdoğan S, et al. Performance of the EuroSCORE II and the STS score for cardiac surgery in octogenarians. Turk Gogus Kalp Damar Cerrahisi Derg. 2021;29:174-182. doi: 10.5606/tgkdc.dergisi.2021.21403
26. Shamkhani W, Rashid M, Moledina S, et al. Complex high-risk percutaneous coronary intervention types, trends, and outcomes in nonsurgical centres. Can J Cardiol. 2024;40:1237-1246. doi: 10.1016/j.cjca.2024.01.003
27. Lee JM, Choi KH, Song YB, et al. Intravascular imaging-guided or angiography-guided complex PCI. N Engl J Med. 2023;388:1668-1679. doi: 10.1056/NEJMoa2216607
28. Khandelwal G, Spirito A, Tanner R, et al. Validation of UK-BCIS CHIP score to predict 1-year outcomes in a contemporary United States population. JACC Cardiovasc Interv. 2023;16:1011-1020. doi: 10.1016/j.jcin.2023.02.005
29. Hirai T, Grantham JA, Sapontis J, et al. Development and validation of a prediction model for angiographic perforation during chronic total occlusion percutaneous coronary intervention: OPEN-CLEAN perforation score. Catheter Cardiovasc Interv. 2022;99:280-285. doi: 10.1002/ccd.29466
30. Simsek B, Kostantinis S, Karacsonyi J, et al. Predicting periprocedural complications in chronic total occlusion percutaneous coronary intervention: the PROGRESS-CTO Complication scores. JACC Cardiovasc Interv. 2022;15:1413-1422. doi: 10.1016/j.jcin.2022.06.007
31. Farooq V, van Klaveren D, Steyerberg EW, et al. Anatomical and clinical characteristics to guide decision making between coronary artery bypass surgery and percutaneous coronary intervention for individual patients: development and validation of SYNTAX score II. Lancet. 2013;381:639-650. doi: 10.1016/S0140-6736(13)60108-7
32. Hanna JM, Wang SY, Kochar A, et al. Complex percutaneous coronary intervention outcomes in older adults. J Am Heart Assoc. 2023;12:e029057. doi: 10.1161/JAHA.122.029057
33. Serruys PW, Morice M-C, Kappetein AP, et al. Percutaneous coronary intervention versus coronary-artery bypass grafting for severe coronary artery disease. N Engl J Med. 2009;360:961-972. doi: 10.1056/NEJMoa0804626
34. Le May M, Wells GA, Chong AY. Do the results of the SYNTAX trial apply to my centre? EuroIntervention. 2017;13:781-783. doi: 10.4244/EIJV13I7A114
35. Ferlini M, Munafò A, Visconti LO. Fractional flow reserve-guided PCI as compared with coronary bypass surgery. N Engl J Med. 2022;386:1865. doi: 10.1056/NEJMc2202491
36. Fearon WF, Zimmermann FM, Ding VY, et al. Quality of life after fractional flow reserve–guided PCI compared with coronary bypass surgery. Circulation. 2022;145:1655-1662. doi: 10.1161/CIRCULATIONAHA.122.060049
37. Shin D, Karimi Galougahi K, et al. Calcified nodule in percutaneous coronary intervention. JACC Cardiovasc Interv. 2024;17:1187-1199. doi: 10.1016/j.jcin.2024.03.032
38. Yeh RW, Secemsky EA, Kereiakes DJ, et al. Development and validation of a prediction rule for benefit and harm of dual antiplatelet therapy beyond 1 year after percutaneous coronary intervention. JAMA. 2016;315:1735-1749. doi: 10.1001/jama.2016.3775
39. Costa F, van Klaveren D, James S, et al. Derivation and validation of the predicting bleeding complications in patients undergoing stent implantation and subsequent dual antiplatelet therapy (PRECISE-DAPT) score: a pooled analysis of individual-patient datasets from clinical trials. Lancet. 2017;389:1025-1034. doi: 10.1016/S0140-6736(17)30397-5
40. Baber U, Mehran R, Giustino G, et al. Coronary thrombosis and major bleeding after PCI with drug-eluting stents: risk scores from PARIS. J Am Coll Cardiol. 2016;67:2224-2234. doi: 10.1016/j.jacc.2016.02.064
41. Urban P, Mehran R, Colleran R, et al. Defining high bleeding risk in patients undergoing percutaneous coronary intervention. Circulation. 2019;140:240-261. doi: 10.1161/CIRCULATIONAHA.119.040167
42. Xenogiannis I, Varlamos C, Keeble TR, et al. Ultrasound-guided femoral vascular access for percutaneous coronary and structural interventions. Diagnostics (Basel). 2023;13:2028. doi: 10.3390/diagnostics13122028
43. Jolly SS, AlRashidi S, d’Entremont M-A, et al. Routine ultrasonography guidance for femoral vascular access for cardiac procedures: the UNIVERSAL randomized clinical trial. JAMA Cardiol. 2022;7:1110-1118. doi: 10.1001/jamacardio.2022.3399
44. StatPearls [Internet]. StatPearls Publishing; 2025. Updated May 7, 2024. https://www.ncbi.nlm.nih.gov/sites/books/NBK535361/
45. Murgic L, Hébert PC, Sovic S, Pavlekovic G. Paternalism and autonomy: views of patients and providers in a transitional (post-communist) country. BMC Med Ethics. 2015;16:65. doi: 10.1186/s12910-015-0059-z
46. Kilbride MK, Joffe S. The new age of patient autonomy: implications for the patient-physician relationship. JAMA. 2018;320:1973-1974. doi: 10.1001/jama.2018.14382
Advertisement
Advertisement
