Advertisement
Advertisement
July/August 2023
Contrast-Enhanced Echocardiography for Evaluating Coronary Artery Perforations
A guide to the use of echocardiography with ultrasound-enhancing agents to aid in the management of coronary artery perforations.
By Jesse A. Kane, MD; Kathleen Kearney, MD; and Jasleen Tiwana, MD
Coronary artery perforations occur in approximately 0.3% to 0.5% of all percutaneous coronary interventions (PCIs) with higher rates in chronic total occlusion (CTO) PCI (4%). Appropriate management of perforations is essential, as they can result in tamponade, hemodynamic collapse, and mortality.1-3 Depending on the severity and anatomy, management of perforations can range from supportive care to emergent cardiac surgery.4 Contrast-enhanced echocardiography (CEE) is a technique that can help guide management strategies in treating these challenging complications.
CEE is an echocardiographic technique that uses ultrasound enhancing agents (UEAs), which are injectable echoreflective microbubbles to improve imaging of the cardiac chambers and blood-filled spaces. In the setting of perforations, these microbubbles better characterize the perforation. UEAs can differentiate if there is blood extravasation into the pericardium or into a cardiac chamber. They can also be utilized to better decipher whether there is ongoing bleeding or if a perforation has sealed.
HOW TO DO IT
The technique, as subsequently described, is performed in the cath lab with UEA injected via a guide catheter directly into the coronary artery. However, CEE is also valuable once the patient has left the lab and can be performed via peripheral intravenous (IV) access in the standard fashion.
Communicate With Your Echocardiographer
Ensure that there are adequate windows to assess the region of interest (eg, ensure the anterior wall pericardium can be seen well in the setting of a left anterior descending perforation).
Ensure the Ultrasound Machine Is Appropriately Set for Imaging of the UEA
Reduce the mechanic index to avoid destruction of microbubbles and follow manufacturer recommended settings/institutional guidelines to provide optimal imaging.5
Dilute the UEA
Dilute according to standard protocol for your institution based on the brand of UEA available in your lab. The dilution is the same regardless of injection via the coronary guide catheter or peripheral IV.
Perform Intracoronary Injection of the UEA and Record Ultrasound Images
Inject 1 to 2 mL of the diluted UEA via the guide catheter into the coronary artery and follow with a slow normal saline flush (over approximately 10 seconds) while recording the images. Too fast of an injection can cause shadowing and obstruct imaging.
Review Images
Review the recorded images and consider multiple views to ensure the pericardium is well visualized.
Evaluate Results
If ongoing bleeding is seen on angiography and UEA is present in the pericardium, it is consistent with a coronary perforation into the pericardium. If ongoing bleeding is seen on angiography, but UEA does not fill the pericardium, look for filling of the cardiac chambers, this is consistent with bleeding into a cardiac chamber or coronary vein. If the bleeding is not seen on angiography and UEA does not fill the pericardium, look for filling of the cardiac chambers, which is indicative of a sealed perforation.
EXAMPLES OF THE TECHNIQUE
Case 1
A woman in her late 60s with a history of coronary artery disease presented for proximal left anterior descending PCI in the setting of a non-ST-elevation myocardial infarction (Figure 1A). The procedure was complicated by a distal coronary artery perforation caused by a coronary wire (Figure 1B, Video 1). The patient remained hemodynamically stable.
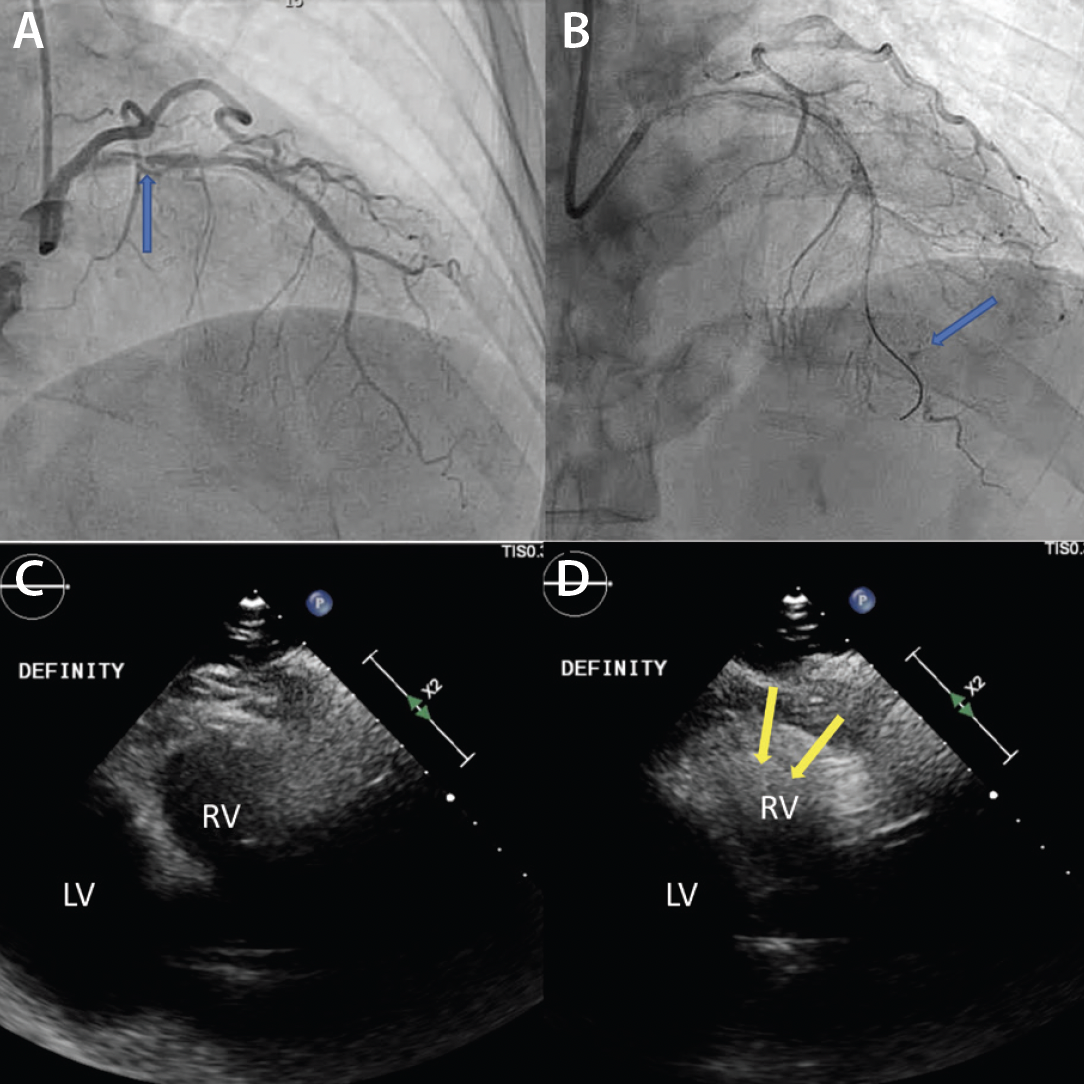
Figure 1. Initial angiography with severe stenosis of the proximal left anterior descending (blue arrow) (A). After intervention, a coronary artery perforation is seen in the distal vessel (blue arrow) (B). Transthoracic echocardiography showing the left ventricle and right ventricle (C). CEE after intracoronary injection of the UEA, the UEA is seen filling the right ventricle while notably absent from the pericardium (D).
Video 1
After balloon tamponade, continued extravasation was present on angiography. CEE was performed with an intracoronary injection of an UEA. The UEA was seen filling the cardiac chambers, but no pericardial effusion was seen and there was no UEA identified filling the pericardial space (Figures 1C and 1D, Video 2). Together with the angiographic finding, we determined the perforation was likely into a coronary vein. No further intervention was performed. The patient remained hemodynamically stable and was later discharged without significant events.
Video 2
Case 2
A man in his late 80s with a history of ischemic cardiomyopathy and angina refractory to optimal medical therapy presented for right coronary artery CTO PCI. The procedure required a retrograde approach via an epicardial collateral, which resulted in a coronary wire perforation of the diagonal branch (Figure 2A, Video 3). Autologous fat embolization was performed via a microcatheter, and the patient remained stable, but it was unclear whether an adequate seal was achieved. CEE was performed with an intracoronary injection of a UEA, revealing UEA filling the pericardium (Figure 2B, Video 4). Ultimately, a pericardial drain was placed and the perforation was sealed with coils.
Video 3
Video 4
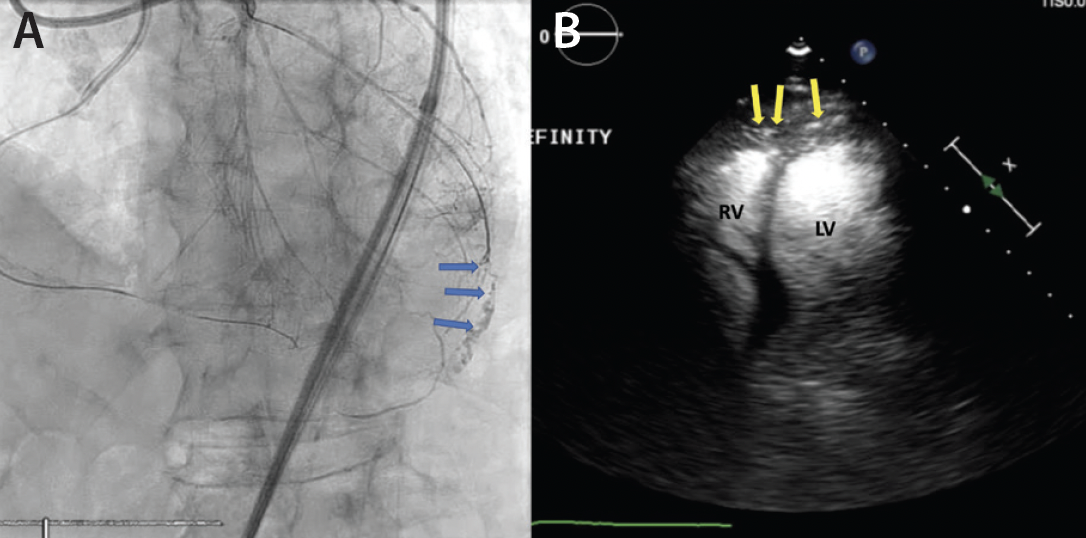
Figure 2. Angiography after retrograde wiring via the epicardial collateral revealing a diagonal branch coronary artery perforation (blue arrows) (A). Transthoracic echocardiography after intracoronary injection of the ultrasound enhancing agent; the radiopaque microbubbles can be seen filling the pericardial space (yellow arrows) suggestive of continued bleeding into the pericardium (B).
KEY CONSIDERATIONS
Hemodynamic Stability
Obtaining CEE can be time consuming and should only be performed when a patient is hemodynamically stable and there is ambiguity regarding the persistence and/or location of the perforation.
Control the Bleeding While Preparing the Images
If there is evidence of active contrast extravasation, temporizing measures such as balloon tamponade should be considered, as tolerated from an ischemic perspective, to prevent clinical decline while further diagnostic information is obtained.
Troubleshooting
If no UEA is seen at all in the CEE, this would be considered a nondiagnostic test. In this setting, ensure the imaging windows are adequate, the UEA has been appropriately diluted and injected, and that the mechanic index of the ultrasound machine has been adjusted.
Outside the Catheterization Lab
CEE should also be considered once the patient has left the lab if there is concern for a pericardial bleed. In this setting, it is important to remember the cardiac chambers will fill with the UEA regardless of the perforation status, but filling seen of UEA in the pericardium is indicative of an on-going pericardial bleed.
Contraindications to UEA
Fortunately, the only contraindication to UEA is an allergy to the components of the selected agent utilized (sulfa hexafluoride, perfluten or blood products depending on the agent used).5
1. Guttmann O, Jones D, Gulati A, et al. Prevalence and outcomes of coronary artery perforation during percutaneous coronary intervention. EuroIntervention. 2017;13:e595-e601. doi: 10.4244/EIJ-D-16-01038
2. Danek BA, Karatasakis A, Tajti P, et al. Incidence, treatment, and outcomes of coronary perforation during chronic total occlusion percutaneous coronary intervention. Am J Cardiol. 2017;120:1285-1292. doi: 10.1016/j.amjcard.2017.07.010
3. Kinnaird T, Kwok CS, Kontopantelis E, et al. Incidence, determinants, and outcomes of coronary perforation during percutaneous coronary intervention in the United Kingdom between 2006 and 2013. Circ Cardiovasc Interv. 2016;9. doi: 10.1161/CIRCINTERVENTIONS.115.003449
4. Abdalwahab A, Farag M, Brilakis ES, et al. Management of coronary artery perforation. Cardiovasc Revasc Med. 2021;26:55-60. doi: 10.1016/j.carrev.2020.11.013
5. Porter TR, Mulvagh SL, Abdelmoneim SS, et al. Clinical applications of ultrasonic enhancing agents in echocardiography: 2018 American Society of Echocardiography Guidelines update. J Am Soc Echocardiogr. 2018;31:241-274. doi: 10.1016/j.echo.2017.11.013
Advertisement
Advertisement
