Advertisement
Advertisement
September/October 2022
Catheter-Based Renal Denervation
A review of the evidence for a novel treatment for hypertension.
By Anna K. Krawisz, MD, and Eric A. Secemsky, MD, MSc, RPVI, FACC, FSCAI, FSVM
Hypertension is a major public health concern in the United States and worldwide and is the leading preventable cause of heart attack, stroke, and death.1 Hypertension is pervasive, with nearly 50% of adults affected in the United States. There are significant racial disparities in hypertension, with Black adults disproportionately impacted compared with White and Hispanic adults.2 Of those with hypertension, only 26% have blood pressures that are well controlled.3 Overall, blood pressure control is decreasing in adults in the United States.4 Health care costs associated with hypertension are notably high—estimated to be $131 billion annually.5 As such, it is critical to find novel approaches to managing hypertension.
Catheter-based renal denervation (RDN) is an endovascular, device-based approach for hypertension treatment that shows promise in early clinical trials. RDN works by interrupting the afferent and efferent sympathetic innervation of the renal arteries. The effects of this are to reduce vascular resistance, renin release, and sodium reabsorption.6,7 This therapy offers a unique alternative to medications for patients who may struggle with side effects of medications or with adherence to medications. In addition, RDN is “always on,” such that vulnerable periods of cardiovascular risk, including early in the morning, have consistent hypertension control. Currently, these devices are not FDA approved, but multiple trials have demonstrated their efficacy in blood pressure lowering.
evidence REVIEW
Symplicity Spyral
Two recent randomized, single-blind, sham-controlled trials of the Symplicity Spyral multielectrode catheter (Medtronic) have demonstrated clinically significant reductions in blood pressure: the SPYRAL HTN-OFF MED pivotal and SPYRAL HTN-ON MED pilot trials (Figure 1).8,9 The Spyral device uses radiofrequency energy to ablate nerves through thermal damage.
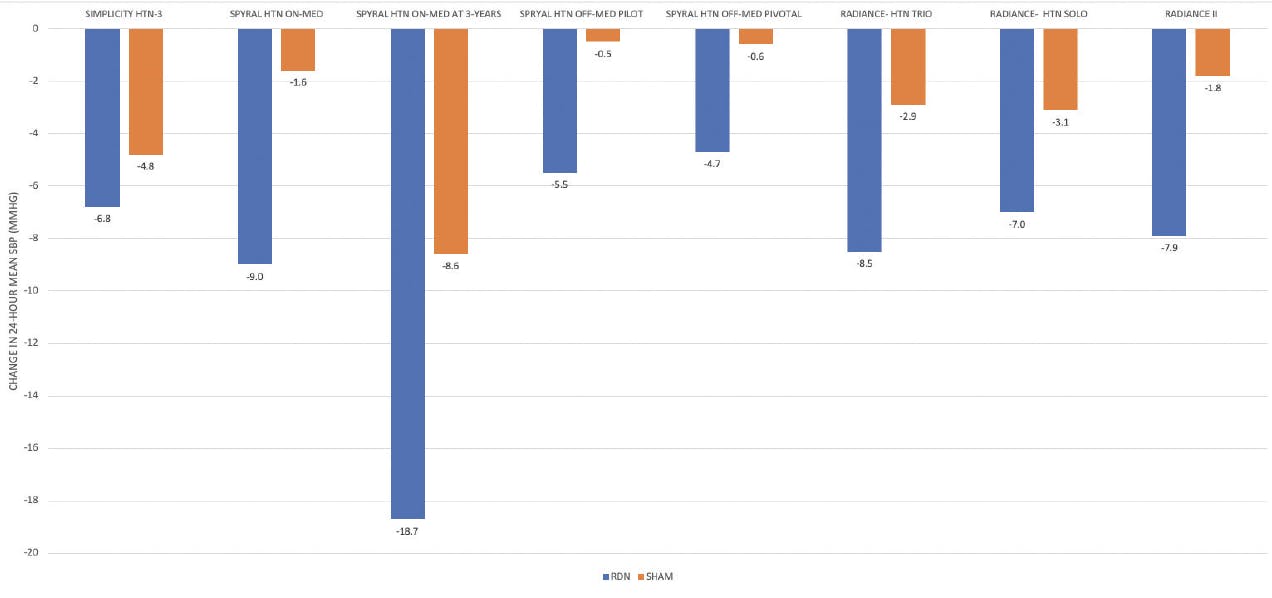
Figure 1. Change in 24-hour mean SBPs in RDN compared with sham control in key device trials and registries. RDN reduces blood pressure in different patient populations, across device platforms, and at 3 years of follow-up. (Adapted from Kandzari DE, Townsend RR, Bakris G, et al. Renal denervation in hypertension patients: proceedings from an expert consensus roundtable cosponsored by SCAI and NKF. Catheter Cardiovasc Interv. 2021;98:416-426).
SPYRAL HTN-OFF MED. The SPYRAL HTN-OFF MED pivotal trial included 21 centers in the United States, Europe, Japan, and Australia.8 Patients had office systolic blood pressure (SBP) in the range of 150 to 179 mm Hg, diastolic blood pressure ≥ 90 mm Hg, and 24-hour systolic ambulatory blood pressure of 140 to 169 mm Hg and were not on antihypertensive medication. After renal angiography, patients were randomly assigned to either a RDN or sham control group. In those who underwent RDN, the trial found significant reductions in 24-hour ambulatory blood pressures at 3 months (treatment difference, –4.0 mm Hg; 95% CI, –6.2 to –1.8; P = .0005) (Figure 1).10 Due to patients not taking their antihypertensive medication, this study also included escape criteria for those patients whose office SBP reached ≥ 180 mm Hg. A significantly higher number of patients from the sham arm reached the escape criteria compared to the RDN group (15 vs 7; P = .046).11
SPYRAL HTN-ON MED. The SPYRAL HTN-ON MED pilot trial similarly demonstrated the efficacy of RDN in lowering blood pressure but in patients on antihypertensive medications.9 Patients with the same blood pressure parameters in the SPYRAL HTN-OFF MED trial who were on stable blood pressure regimens consisting of one to three medications were enrolled. Patients were maintained on their antihypertensive medications throughout the trial. At 6 months, those who underwent RDN experienced a significantly greater decrease in 24-hour ambulatory systolic BP (–9.0 mm Hg; 95% CI: –12.7 to –5.3 mm Hg; P < .0001) relative to those assigned to sham control (–1.6 mm Hg; 95% CI: –5.2 to 2.0 mm Hg; P = .365; baseline adjusted difference between groups –7 mm Hg; 95% CI: –12.0 to –2.1; P = .0059). Medication changes were permitted at 6 months. At 12 months, physicians were unblinded, and crossover was allowed. At 3 years, the success of RDN treatment was sustained. There was a 10 mm Hg greater reduction in 24-hour SBP in patients who underwent RDN relative to sham control at 3 years, which is a statistically significant result. In addition, there were significant reductions in morning, daytime, and nighttime SBPs in the RDN group.12 The percentage of patients who had 24-hour SBP of ≤ 140 mm Hg was significantly greater in the RDN arm (83.3% vs 43.8%; P = .0002). Fewer medications were used by the RDN group relative to the sham group, but this difference was not statistically significant.
Global SYMPLICITY Registry. This RDN system was further evaluated in the Global SYMPLICITY registry (US National Library of Medicine. clinicaltrials.gov; https://clinicaltrials.gov/ct2/show/NCT01534299 [2019]), which is a prospective, open-label, single-arm, multicenter observational study with data from 196 sites worldwide. This data set was created to evaluate longer-term durability and safety, high-risk subgroup populations, and patients from a real-world setting. It included 2,652 patients with uncontrolled hypertension who were treated with the Symplicity Flex or Spyral devices. The evaluated subgroups included resistant hypertension, isolated systolic hypertension, chronic kidney disease, patients aged 65 years or older, atrial fibrillation, and patients with high cardiovascular risk scores. The registry has demonstrated significant blood pressure reductions in all subgroups at 6 months, which were sustained at 3 years of follow-up. RDN was associated with a 26% relative risk reduction in major adverse cardiac events.13
Paradise
RADIANCE-HTN SOLO. Endovascular RDN devices that function by using ultrasound to disrupt renal innervation have also been shown to be effective in reducing blood pressures. The Paradise catheter system (ReCor Medical) was tested in the RADIANCE-HTN SOLO trial, a multicenter, sham-controlled trial.14 This trial was powered to show superiority of RDN over the sham procedure in lowering daytime ambulatory SBPs. Patients with systolic-diastolic hypertension with daytime ambulatory SBPs in the 135 to 169 mm Hg range and diastolic blood pressures in the 85 to 104 mm Hg range after discontinuing up to two antihypertensive medications were randomly assigned to RDN or a sham procedure. At 2 months, there was a significant reduction in daytime ambulatory blood pressure in the RDN group (–8.5 ± 9.3 mm Hg) compared with the sham control group (–2.2 ± 10.0 mm Hg; baseline-adjusted difference between groups −6.3 mm Hg; 95% CI, −9.4 to −3.1 mm Hg; P = .0001). At 6 months, the blood pressure–lowering efficacy of RDN persisted.15 Fewer antihypertensive medications were required to achieve the same blood pressure–lowering effect in the RDN group compared with the sham control group, and significantly more patients in the RDN group did not require any antihypertensive medications at 6 months compared with the sham control group.15 At 36 months of follow-up, the effectiveness of RDN was sustained.16
RADIANCE-HTN TRIO. The RADIANCE-HTN TRIO trial evaluated ultrasound RDN in patients with resistant hypertension.17 This was a randomized, multicenter, single-blind, sham-controlled trial that included 53 centers in the United States and Europe. Patients were enrolled who had blood pressure of 140/90 mm Hg despite three or more antihypertensive medications, including a diuretic. All patients were treated with a standardized medication regimen of a fixed-dose combination pill combining a calcium channel blocker, an angiotensin receptor blocker, and a thiazide diuretic. Patients with daytime ambulatory blood pressures of ≥ 135/85 mm Hg were then randomized to ultrasound RDN or sham procedure. There was a significant reduction in daytime ambulatory SBP in patients who underwent RDN compared with sham (−8.0 mm Hg [IQR, −16.4 to 0.0] vs −3.0 mm Hg [IQR, −10.3 to 1.8]; median between-group difference, −4.5 mm Hg [95% CI, −8.5 to −0.3]; adjusted P = .022).
RADIANCE II. The RADIANCE II trial further evaluated the safety and efficacy of ultrasound-based RDN (ReCor Medical Paradise System) in patients with uncontrolled hypertension on zero to two antihypertensive medications. Two hundred twenty-four patients were randomized to either RDN or a sham procedure. All antihypertensive medications were discontinued prior to randomization. At 2 months, RDN resulted in a greater reduction in ambulatory systolic BP (–7.9 mm Hg) compared with sham procedure (–1.8 mm Hg; between-group difference –6.3 mm Hg; 95% CI: –9.3 to –3.2 mm Hg; P < .0001).18
RESULTS
The data available thus far regarding RDN are reassuring in terms of safety. No long-term safety concerns have been identified. More specifically, in the RADIANCE-HTN SOLO trial, there was one transient ischemic attack at 458 days after RDN, one hypertensive event at 1,076 days after RDN, and one patient with renal artery stenosis with stent placement 6 months postprocedure.16 No events were identified as being related to the device or procedure. No patients developed acute renal injury, end-stage renal disease, or renal artery complications requiring reintervention (eg, dissection, perforation) at 3-year follow-up. In the SPYRAL HTN-ON MED trial, there was one death in the sham arm. In the RDN arm, there was one hospitalization for hypertensive crisis/emergency and one stroke. Importantly, after 3 years, there were no new renal artery stenoses, renal artery reinterventions, elevations of creatinine above 50%, or new-onset end-stage renal disease.12
CONCLUSION
Overall, RDN presents a potentially exciting therapy with which to combat the worldwide epidemic of hypertension. An emerging body of evidence demonstrates the ability of RDN to effectively reduce blood pressure over time in multiple patient subgroups and via different device platforms (Figure 1).19 RDN may combat several major barriers to successful treatment of patients with hypertension, such as adherence and medication side effects. There are several critical questions remaining, such as optimal patient selection, length of blood pressure–lowering effects with RDN, long-term safety, and delineating specific mechanisms of blood pressure reduction.7
1. Bundy JD, Mills KT, Chen J, et al. Estimating the association of the 2017 and 2014 hypertension guidelines with cardiovascular events and deaths in US adults: an analysis of national data. JAMA Cardiol. 2018;3:572-581. doi: 10.1001/jamacardio.2018.1240
2. Ostchega Y, Nguyen DT. Hypertension prevalence among adults aged 18 and over: United States, 2017–2018. NCHS Data Brief. 2020;:8.
3. Centers for Disease Control and Prevention. Facts about hypertension. Published September 27, 2021. Accessed March 1, 2022. https://www.cdc.gov/bloodpressure/facts.htm
4. Muntner P, Hardy ST, Fine LJ, et al. Trends in blood pressure control among US adults with hypertension, 1999-2000 to 2017-2018. JAMA. 2020;324:1190-1200. doi: 10.1001/jama.2020.14545
5. Kirkland EB, Heincelman M, Bishu KG, et al. Trends in healthcare expenditures among US adults with hypertension: national estimates, 2003–2014. J Am Heart Assoc. 2018;7:e008731. doi: 10.1161/JAHA.118.008731
6. Lauder L, Azizi M, Kirtane AJ, et al. Device-based therapies for arterial hypertension. Nat Rev Cardiol. 2020;17:614-628. doi: 10.1038/s41569-020-0364-1
7. Kiuchi MG, Esler MD, Fink GD, et al. Renal denervation update from the International Sympathetic Nervous System Summit. J Am Coll Cardiol. 2019;73:3006-3017. doi: 10.1016/j.jacc.2019.04.015
8. Townsend RR, Mahfoud F, Kandzari DE, et al. Catheter-based renal denervation in patients with uncontrolled hypertension in the absence of antihypertensive medications (SPYRAL HTN-OFF MED): a randomised, sham-controlled, proof-of-concept trial. The Lancet. 2017;390:2160-2170. doi: 10.1016/S0140-6736(17)32281-X
9. Kandzari DE, Böhm M, Mahfoud F, et al. Effect of renal denervation on blood pressure in the presence of antihypertensive drugs: 6-month efficacy and safety results from the SPYRAL HTN-ON MED proof-of-concept randomised trial. The Lancet. 2018;391:2346-2355. doi: 10.1016/S0140-6736(18)30951-6
10. Böhm M, Kario K, Kandzari DE, et al; SPYRAL HTN-OFF MED Pivotal Investigators. Efficacy of catheter-based renal denervation in the absence of antihypertensive medications (SPYRAL HTN-OFF MED pivotal): a multicentre, randomised, sham-controlled trial. Lancet. 2020;395:1444-1451. doi: 10.1016/S0140-6736(20)30554-7
11. Weber MA, Schmieder RE, Kandzari DE, et al. Hypertension urgencies in the SPYRAL HTN-OFF MED Pivotal trial. Clin Res Cardiol. Published online July 19, 2022. doi: 10.1007/s00392-022-02064-5
12. tctMD. SPYRAL HTN-ON MED at 3 years: renal denervation’s BP impact endures. Accessed August 22, 2022. https://www.tctmd.com/news/spyral-htn-med-3-years-renal-denervations-bp-impact-endures
13. Mahfoud F, et al. Effects of renal denervation on kidney function and long-term outcomes: 3-year follow-up from the Global SYMPLICITY Registry. Presented at the TCT 2022 annual meeting; Boston, Massachusetts, MA; September, 19-21, 2022.
14. Azizi M, Schmieder RE, Mahfoud F, et al. Endovascular ultrasound renal denervation to treat hypertension (RADIANCE-HTN SOLO): a multicentre, international, single-blind, randomised, sham-controlled trial. The Lancet. 2018;391:2335-2345. doi: 10.1016/S0140-6736(18)31082-1
15. Azizi M, Schmieder RE, Mahfoud F, et al. Six-month results of treatment-blinded medication titration for hypertension control after randomization to endovascular ultrasound renal denervation or a sham procedure in the RADIANCE-HTN SOLO Trial. Circulation. 2019;139:2542-2553. doi: 10.1161/CIRCULATIONAHA.119.040451
16. Rader F, Kirtane AJ, Wang Y, et al. Durability of blood pressure reduction after ultrasound renal denervation: three-year follow-up of the treatment arm of the randomised RADIANCE-HTN SOLO trial. EuroIntervention. Published online August 1, 2022. doi: 10.4244/EIJ-D-22-00305
17. Azizi M, Sanghvi K, Saxena M, et al. Ultrasound renal denervation for hypertension resistant to a triple medication pill (RADIANCE-HTN TRIO): a randomised, multicentre, single-blind, sham-controlled trial. The Lancet. 2021;397:2476-2486. doi: 10.1016/S0140-6736(21)00788-1
18. Kirtane AJ. Presented by at the Transcatheter Cardiovascular Therapeutics annual meeting, Boston, MA; September 18, 2022.
19. Kandzari DE, Townsend RR, Bakris G, et al. Renal denervation in hypertension patients: Proceedings from an expert consensus roundtable cosponsored by SCAI and NKF. Catheter Cardiovasc Interv. 2021;98:416-426. doi: 10.1002/ccd.29884
Advertisement
Advertisement
