Advertisement
Advertisement
September/October 2021
Dual Lumen Catheters: When and How to Use Them
Techniques for increasingly complex PCI.
The complexity of percutaneous coronary intervention (PCI) in the current era has increased significantly. Patients undergoing PCI are older, have more comorbidities, prior coronary bypass grafts, and more heavily calcified and tortuous lesions that often involve coronary bifurcations. Additionally, there has been an uptake in the treatment of chronic total occlusions (CTOs), which pose a particular challenge for percutaneous revascularization as opposed to bypass. The use of novel techniques and devices, such as microcatheters, has become essential in increasing the success rate of these more complex interventions.1 Dual lumen microcatheters (DLMs) have recently been introduced to further facilitate PCI of complex anatomy. Several DLMs are currently available and the role for their utilization is expanding. Each device has unique design characteristics. However, all share the common feature of two distinct lumens to facilitate the precise handling of two separate guidewires.2 This article focuses on the currently available DLMs and their applications. Please also see the article by Dr. Martins Filho from this issue for additional reading.
WHY I DO IT
The role for DLMs is expanding and will likely continue to grow with the increase in complexity of PCI. Their application is most useful in the setting of PCI for bifurcation lesions, CTOs, and a combination of the two (Table 1).

Bifurcations
Coronary bifurcation PCI accounts for approximately 20% of all PCI procedures and is associated with increased procedural cost, higher complication rates, and worse outcomes.3 It remains one of the most challenging subsets of lesions, often due to difficulty in wiring of the side branch. DLMs can be particularly helpful in challenging side branch wiring due to highly angulated (angles ≥ 150°) side branches, or those with unfavorable take-off angles when conventional wiring techniques have failed. In this instance, a microcatheter-assisted reverse wire (RW) technique can be employed to facilitate wiring of the side branch. This technique was first developed by Kawasaki et al in 2008,4 but it has been modified to incorporate DLMs to facilitate wiring of narrow, angulated side branches. DLMs can also provide additional support when rewiring difficult side branches through prior stent struts.
Chronic Total Occlusions
CTOs still represent one of the most challenging lesion subsets for percutaneous intervention. The technical success of CTO PCI has improved recently due to the development of novel techniques and devices,1,5 however, the inability to cross the CTO remains the most common cause of failure.5 The presence of bifurcation lesions in the context of CTO, which occurs occasionally, increases the complexity of these lesions greatly.6 DLMs have several useful applications when employed in the context of CTO PCI (Table 1). DLMs may be helpful when a parallel wire technique is needed during antegrade CTO PCI. In this scenario, the subintimal wire (through the rapid-exchange [RX] port) acts as a guide and provides support to the second working wire (through the over the wire [OTW] port) that can be manipulated to find the true lumen.
MATERIALS
There are currently five DLMs available in the United States and FDA approved for coronary use: Twinpass and Twinpass Torque (Teleflex), NHancer Rx (IMDS), Sasuke (Asahi Intecc USA, Inc.), and ReCross (IMDS). Two additional DLMs are currently available outside the United States: FineDuo (Terumo Europe) and the Crusade (Kaneka Medical Products). Most contemporary DLMs have both an RX lumen, in which the distal port is at the distal tip of the catheter, and an OTW lumen, in which the distal port is located more proximally. The distance from the catheter tip (RX port) and OTW port varies depending on the catheter. Two radiopaque markers are positioned to identify the exit ports of both lumens. All current DLMs are compatible with 5-F guiding catheters and have a hydrophilic coating to improve delivery.
Table 2 summarizes the major characteristics and differences between available DLMs. The Twinpass Torque microcatheter has a stainless-steel braided shaft designed to enhance torque control and deliverability. The NHancer Rx’s distal shaft design provides the smallest dual lumen crossing profile (2.3 F), allowing for catheter trapping using a conventional balloon in a 6-F guide. The ReCross microcatheter is the only DLM with two OTW lumens, making guidewire exchange possible through both lumens. Additionally, one of the two OTW lumens has two exit ports located 180° apart. This unique feature allows for advancing guidewires in multiple directions, which can facilitate true lumen reentry in the case of subintimal guidewire crossing. DLMs with a larger outer diameter have larger crossing profiles but in return enhance back-up and stability.

HOW I DO IT
All current DLMs are compatible with the standard 6-F guiding catheters and can accommodate 0.014-inch guiding wires through both the RX and OTW ports. Larger-bore guiding catheters (≥ 7 F) should be considered to provide additional support to allow larger device delivery and facilitate adjunctive maneuvers such as the trapping balloon technique and atherectomy.
Step-by-Step Approach
Step 1: Prepare lesion to aid in advancement and proper positioning. Because DLMs are slightly larger profile than standard coronary microcatheters, predilation may be necessary to facilitate delivery and proper positioning of the OTW exit port.
Step 2: Advance DLM over guidewire. DLMs are advanced over 0.014-inch guidewire through the RX lumen similarly to standard RX devices. The distal tip of the RX lumen is located at the distal tip of the catheter.
Step 3: Position. Once the catheter is in place, it can then be positioned such that the radiopaque marker identifying the OTW exit port is situated at the site where precise wiring is needed (Figure 1, Video 1). In the case of bifurcations, one would position this at the origin of the side branch of interest. DLM selection should take into consideration the angle and distance between the branch of interest and the main vessel because the currently available DLMs have varying distances between the OTW lumen distal port and the tip of the catheter (RX port).
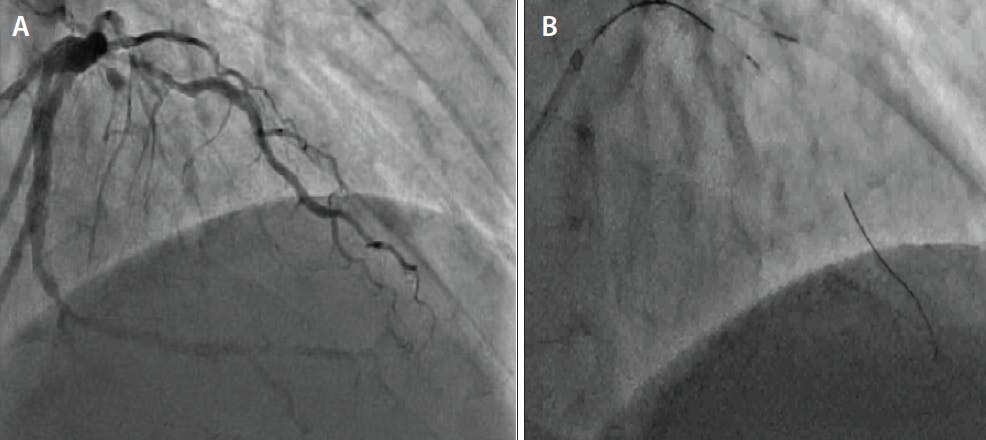
Figure 1. Pre-PCI angiography demonstrates bifurcation CTO disease involving a large first diagonal artery with proximal stenosis and mid left anterior descending (LAD) artery CTO with left-to-left, septal-to-septal, and diagonal-to-diagonal collaterals (Video 1) (A). The CTO was crossed with antegrade dissection reentry into the second diagonal. In this still frame, there is a wire positioned in the distal second diagonal. A microcatheter is positioned in the first diagonal that was used for visualization of collaterals to the LAD artery and second diagonal. The second diagonal takeoff was near the distal CTO cap. A Sasuke DLM with the OTW port was positioned at the CTO distal cap to access the LAD (B).
Video 1
Step 4: Wire branch/lesion of interest. With the DLM in proper position, one can more precisely steer the guidewire into the area of interest. Careful manipulation of the DLM forward/backward and/or rotating the device and then advancing the wire can facilitate finding the correct origin of the target vessel (Figure 2, Video 2).

Figure 2. Still frame depicting successful wiring of a LAD artery CTO using the Sasuke DLM (A). Final results after successful CTO intervention with bifurcation stenting to the LAD and diagonal (Video 2) (B).
Video 2
Step 5: Remove DLM. Once the guidewire in the OTW port has successfully been placed in the target vessel, the DLM should ideally be removed with a trapping balloon technique to minimize guidewire movement. With the trapping technique, the DLM is withdrawn into the guide catheter. Next, a balloon is advanced into the distal portion of the guide catheter. Either a standard compliant balloon or special trap balloon is advanced into the guiding catheter rather than over a wire, distal to the DLM. The balloon is inflated to 14 atm to “trap” the wire against the wall of the guide catheter, guide pressure will damp (an abrupt reduction in the aortic pressure tracing) indicating an occlusive seal, and the microcatheter can be removed without wire manipulation. Alternatively, the DLM can be removed via the hydraulic technique, using OTW or a wire extension for short wires. Once removed, the DLM can be replaced with a workhorse microcatheter as needed.
TECHNIQUES FOR SPECIFIC ANATOMY
RW Technique
The RW technique was originally developed by Kawasaki et al in 20084 but has been modified to incorporate DLM to facilitate wiring of narrow, angulated side branches. In the RW technique, a preshaped RW, which contains two bends (“swan-neck” shape) is inserted into the OTW lumen of the DLM. The DLM is then inserted into the main vessel through the RX port beyond the bifurcation. The tip of the RW in the OTW lumen is then directed toward the side branch of interest. Both the DLM and RW are then pulled back to engage the origin of the side branch facilitating wiring.7
Parallel Wire Technique
The parallel wire technique was first described by Reifart in 1995 (Reifart N, The parallel wire technique for chronic total occlusions. Interventional Course Frankfurt, 1995; personal communication) and is a useful technique to access the true lumen in CTO PCI when initial wiring attempts are subintimal. DLMs can be helpful in aiding this technique. The DLM is advanced over the subintimal wire via the RX lumen. The catheter is positioned proximal to where the first wire entered the subintimal space. A second guidewire can then be advanced through the OTW lumen and the parallel wire technique employed.
Antegrade Wiring of CTO With Adjacent Side Branch
One of the most unfavorable anatomic features for antegrade CTO PCI is having a side branch adjacent to the proximal or distal caps.6 Use of a DLM can assist in improving precise manipulation of the guidewire into the proximal cap. A DLM is advanced in a side branch until the lateral port is at the level of the proximal cap. A CTO dedicated guidewire can then be advanced through the OTW lumen to engage the occlusion. This not only allows precise handling of the CTO guidewire but also enhances backup to facilitate the proximal cap puncture. Additionally, because it is positioned in the OTW lumen, the CTO dedicated guidewire can be advanced safely up to the level of the proximal cap.8 A DLM can be used when a CTO wire reenters a branch at the distal cap. The OTW lumen can be positioned to allow true lumen wiring or antegrade dissection reentry into the main vessel. An example of use of DLMs for main vessel access after CTO wired into a side branch is presented in Figure 1 and Figure 2.
Additional Techniques for Retrograde CTO PCI
DLMs can also facilitate antegrade CTO crossing when retrograde interventional collaterals are close to the distal cap of the CTO. In this circumstance, once the CTO is traversed in a retrograde fashion and the guidewire is externalized, the retrograde microcatheter is withdrawn inside the collateral. A DLM is then advanced antegrade on the externalized guidewire until the proximal marker is at the level of interlink of the interventional collateral with the distal target vessel. A second workhorse guidewire is then advanced through the OTW lumen of the DLM to wire the true lumen of the vessel distally.2,6,8
A side branch adjacent to the distal cap of a CTO is another unfavorable anatomic feature for retrograde CTO PCI.6 DLMs can also be used to wire the distal true lumen without losing access to a distal side branch near the distal cap of a CTO. A DLM can be advanced through the collateral channel over a wire positioned in the side branch until the lateral port is at the level of the distal cap, where a dedicated CTO wire can then be used through the OTW lumen to engage the occlusion.2,6,8
COMPLICATIONS
Complications and failure modes of commonly used microcatheters have not been evaluated robustly. One study that systematically reviewed data from the MAUDE database found that the most commonly reported microcatheter failure mode was tip fracture (80.7%). This was most commonly due to overtorquing or forceful pulling of the microcatheter after it became entrapped in a lesion.9 Understanding how to advance microcatheters is certainly critical for optimal and safe use. Newer devices provide stronger support of the microcatheter tip, decreasing the likelihood of tip detachment or deformation.
1. Patel VG, Brayton KM, Tamayo A, et al. Angiographic success and procedural complications in patients undergoing percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 18,061 patients from 65 studies. JACC: Cardiovasc Interv. 2013;6:128-136. doi: 10.1016/j.jcin.2012.10.011.
2. Oreglia JA, Garbo R, Gagnor A, et al. Dual lumen microcatheters for complex percutaneous coronary interventions. Cardiovasc Revasc Med. 2018;19:298-305. doi: 10.1016/j.carrev.2017.09.016
3. Lassen JF, Holm NR, Banning A, et al. Percutaneous coronary intervention for coronary bifurcation disease: 11th consensus document from the European Bifurcation Club. Eurointervention. 2016;12:38-46. doi: 10.4244/EIJV12I1A7
4. Kawasaki T, Koga H, Serikawa T. New bifurcation guidewire technique: a reversed guidewire technique for extremely angulated bifurcation--a case report. Catheter Cardiovasc Interv. 2008;71:78-76. doi: 10.1002/ccd.21297
5. Sapontis J, Christopoulos G, Grantham JA, et al., Procedural failure of chronic total occlusion percutaneous coronary intervention: insights from a multicenter US registry. Catheter Cardiovasc Interv. 2015;85:1115-1122. doi: 10.1002/ccd.25807
6. Galassi AR, Boukhris M, Tomasello SD, et al. Incidence, treatment, and in-hospital outcome of bifurcation lesions in patients under- going percutaneous coronary interventions for chronic total occlusions. Coron Artery Dis. 2015;26:142-149. doi: 10.1097/MCA.0000000000000194
7. Hasegawa K, Yamamoto W, Nakabayashi S, Otsuji S. Streamlined reverse wire technique for the treatment of complex bifurcated lesions. Catheter Cardiovasc Interv. 2020;96:E287-E291. doi: 10.1002/ccd.28656
8. Sianos G, Werner GS, Galassi AR, et al. Recanalisation of chronic total coronary occlusions: 2012 consensus document from the EuroCTO club. EuroIntervention. 2012;8:139-145. doi: 10.4244/EIJV8I1A21
9. Megaly M, Sedhom R, Pershad A, et al. Complications and failure modes of coronary microcatheters: Insights from the manufacturer and user facility device experience (MAUDE) database. EuroIntervention. Published online July 7, 2020. doi: 10.4244/EIJ-D-20-0057
Advertisement
Advertisement
